身體數據庫補足最後一哩!AI智慧醫療崛起
張殿文 2018.03.01
.jpg)
隨著人體數據庫資料越來越完善,下一個要起飛的人工智慧應用領域就在:醫療。
去年底,蘋果營運長威廉斯(Jeff Williams)來台參加台積電30週年紀念會,指出醫療生技將是蘋果未來十年大計,因感測元件的技術突破,讓Apple Watch成了智慧醫療先鋒。然而,這只是蘋果布局智慧醫療的一小部分,也僅是眾多跨足智慧醫療的科技巨頭其中一員。與其說智慧手錶是人工智慧的展現,不如說是人體數據成就了智慧手錶。
近來,愈來愈多科學家和創業者相繼投入健康(Health)、人工智慧(AI)結合的新藍海「AIoH」,從基因編輯到感測晶片,瞄準人類各種病症變化。台大癌中心院長鄭安理認為,現今人工智慧高度發展,未來在醫療領域的應用也更加值得期待。
MIT研究員張鋒指出,若是沒有數位科技的運算演進、精確顯示,有些醫學層面的突破相當困難,基因工程研究就是一例。現在,基因已經可以透過「編輯」,讓結構重新轉變,使得基因研究進入新階段。
無獨有偶,台大分子生醫影像研究中心主任曾文毅就是用人工智慧的影像辨識技術,判讀人類1千億個神經元細胞的連結通路,並且偵測神經纖維的方向及長度,進而防止各種腦部病變。
身體就是五感AI使用介面
伴隨人工智慧的技術突破,舉凡人體最重要的五種接受器──眼、耳、鼻、舌、身,都可以透過智慧裝置感測,並把抽象的色、聲、香、味、觸,以具體數據呈現。像工研院開發的電子鼻,從受試者呼出的氣體中,是否含有較多的硫化物、胺類和短鏈脂肪酸,就可朝向尿毒症、肝硬化、肺炎、肺結核四種疾病判別。
愛立信的趨勢研究顯示,身體就是使用者介面(Your Body is the User Interface)的應用趨勢,將在今年變得顯著且重要。
首先,從人類的心跳開始。聯發科打造的全球第一款六合一智慧健康晶片,可蒐集光電容積脈搏波發出的生物信號,僅需約60秒即可測量六項生理數據,適用於早期診斷、預防中風及心臟疾病等等。
其次,由睡眠呼吸切入。為了解決現代人長期睡眠品質不好的問題,大立光結合哈佛醫學院動態生醫指標研究中心ECG技術,成立大立雲康,利用演算法加上心率監測睡眠,在家裡就可進行偵測。
再來,從皮膚開始著手。史丹佛大學團隊發明皮膚癌AI診斷軟體,經過近13萬次測試,結果與21位臨床醫生的專業判斷幾無差異。因影像資料愈來愈多,機器學習技術又不斷進化,提升了圖像辨識準確度。
最後,是最複雜的腦波。由台北科技大學、北醫大共同成立的智慧大腦科技中心,專注發展腦機介面技術,協助漸凍人與外界溝通,未來將結合認知神經科學研究與自駕車科技,期望能降低交通事故發生率。
醫療AI的發展比想像快很多
前Google人工智慧負責人吳恩達表示:「過去AI主要是在資訊技術的領域發揮,未來將會跨越到更多領域應用!」其中,在健康AI上的最新突破,就是利用深度學習方法診斷肺炎,他所發現的演算法可以診斷14種病症,比放射科專家單獨診斷的準確率更高。
李開復則認為,AI的「中期發展」就是應用在醫療產業上。醫療科技之所以排在金融科技後,主要是金融數據的產生和模式沒有阻礙,而醫療領域在這方面還有段路要走。但智慧醫療AI的發展,仍會比家居、汽車更快進入成熟期,因有許多診療服務可用AI替代。
吳恩達和李開復,正是鴻海布局AI的前鋒。不久前,郭台銘在臨時股東會上,意外透露「下一張網」的計畫。他說:「我們的第二張網,就是醫療互聯網!」
健康AI,儼然已成為科技產業最重要的出口。醫療產業是鴻海集團的M次集團所主導,過去鴻海從「3C」到「6C」,從來沒有出現過「M」這個字母,或許一年前,郭台銘都還不確定「醫療物聯網」會這麼重要,將成為全球最大電子製造商的下一張藍圖。
事實上,「網路」結合「醫療」的概念不新,而且阿里巴巴併購了200家診所,還是不得其門而入,但郭台銘敢說醫療是鴻海世代計畫的「第二張網」,說明鴻海已感受到全球科技巨頭的「連動」。
身體數據庫補足AI最後一哩
台北醫大管理學院院長謝邦昌指出,身體發出的信號和診斷紀錄,被台灣的健保制度完整保存下來,「台灣健保」因而成為台灣產業發展下一步的重要利器。面對人口變化,基因科學進步,全民健保這個大數據庫,正好補上醫事在人工智慧的最後一哩。
在全球的醫療數位發展過程之中,原本領先的大廠如IBM、奇異等等,因為大數據時代來臨而重新洗牌,微軟、Google、蘋果等在網路時代急起直追。進入AI時代,大數據庫更加重要,也難怪有人描述,IBM的華生系統雖然在美中最先進的醫療中心布局,但最後還是要與台灣合作,才有用武之地。
健康AI,將掀起新一波醫界改革,在照護體系和新藥開發上,透過導入大數據與機器學習技術,電腦輔助的藥物篩選與設計全面強化,可望縮短新藥開發時程,提高成功機率,新藥開發將邁入「3.0時代」。
除了美國和中國的網路巨頭,韓國也計劃在今年投入百億台幣預算,發展以基因體和腦科學為主的人工智慧,要成為全球製藥和健康照護領域的巨擘。
醫界出身的副總統陳建仁指出,全球人口老化速度加劇,經濟合作暨發展組織(OECD)報告指出生技相關產值將占各先進國家GDP的一半以上,台灣可結合資通訊科技、精密機械與材料的優勢進行布局,以科技啟動全新的健康AI產業,打造新興「兆元」產業。
綜觀而論,沒有什麼產業比得上健康AI,更值得台灣接棒發展了。
數位健康照護產業服務生態概觀
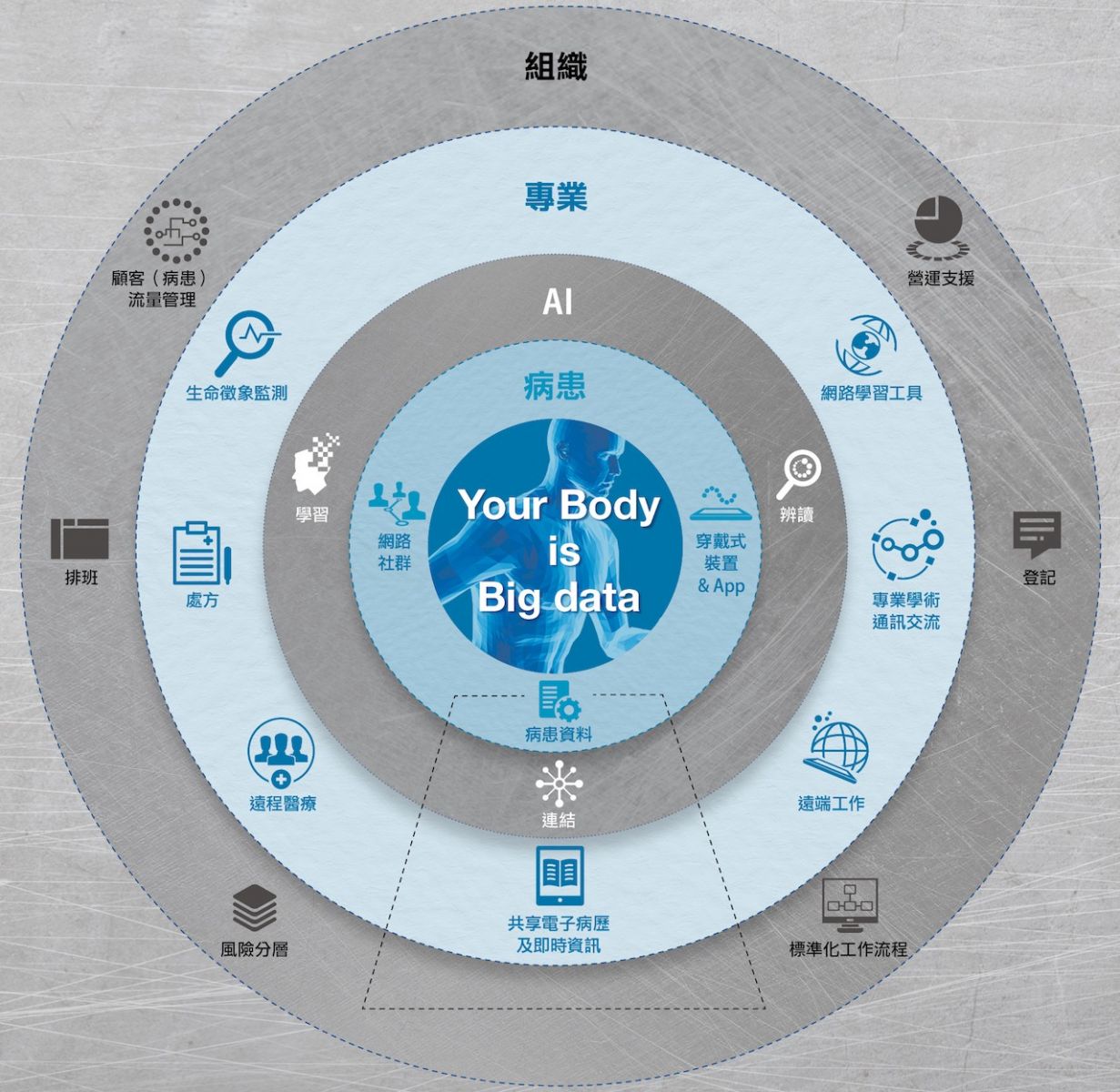
以患者使用的科技軟體為中心,輔以目前進步飛速的人工智慧技術,圓心外的其他科技則根據使用者的不同、提升個別患者照護品質或其改善照護系統的價值差異,而大致歸類為以專業人員為主的科技,以及以組織為主的科技。電子健康紀錄涵蓋整套系統,凸顯其在任何數位策略中都扮演著重要角色。
陳美如、黃巧秀/製作
文章來自: 數位時代
https://www.bnext.com.tw/article/48332/ai-health-care










.jpg)
.jpg)
.jpg)


.jpg)

.jpg)

.jpg)
.jpg)
.jpg)
.jpg)
.jpg)