1 World Health Organization. Dementia: A Public Health Priority. Geneva: World Health Organization; 2012.
2 香港特別行政區立法會:為認知障礙症長者提供的護理服務 ISE10/16-17
3 Yu R, Chau PH, McGhee SM, Cheung WL, Chan KC, Cheung SH and Woo J.(2012) Trends in Prevalence and Mortality of Dementia in Elderly Hong Kong Population: Projections, Disease Burden, and Implications for Long-Term Care. International Journal of Alzheimers Disease. Vol 2012, Article ID 406852.
本周的《自然》雜誌上刊登了一項來自瑞士巴塞爾大學的研究,Michael N. Hall帶領的研究團隊發現了一種全新的抑癌蛋白LHPP,這種蛋白的喪失促進了腫瘤的生長,增加LHPP表達則能夠有效抑制癌細胞增殖並阻止肝功能損傷[1]!除此之外,LHPP水準也與疾病負擔和患者預後有關,研究者認為可以作為診斷和預後的生物指標。
[2] Llovet, J. M. et al. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2,16018–16023 (2016).
[3] Schulze, K. et al. Exome sequencing of hepatocellular carcinomas identifies new mutational signatures and potential therapeutic targets. Nat. Genet. 47,505–511 (2015).
[4] Kenerson, H. L. et al. Akt and mTORC1 have different roles during liver tumorigenesis in mice. Gastroenterology 144, 1055–1065 (2013).
[5] Guri, Y. et al. mTORC2 promotes tumorigenesis via lipid synthesis. Cancer Cell 32, 807–823 (2017).
[6] Makowska, Z. et al. Gene expression analysis of biopsy samples reveals critical limitations of transcriptome-based molecular classifcations of hepatocellular carcinoma. J. Pathol. Clin. Res. 2, 80–92 (2016).
[7] Vogelstein, B. et al. Cancer genome landscapes. Science 339, 1546–1558(2013).
[8] Vijayakrishnan, J. et al. A genome-wide association study identifes risk loci for childhood acute lymphoblastic leukemia at 10q26.13 and 12q23.1. Leukemia 31, 573–579 (2017).
[9] Lesseur, C. et al. Genome-wide association analyses identify new susceptibility loci for oral cavity and pharyngeal cancer. Nat. Genet. 48, 1544–1550 (2016).
Scanning electron microscopy image of cancer cells. Credit: University of Basel, Biozentrum/Swiss Nanoscience Institute
An international team of researchers has discovered a new anti-cancer protein. The protein, called LHPP, prevents the uncontrolled proliferation of cancer cells in the liver. The researchers led by Prof. Michael N. Hall from the Biozentrum, University of Basel, report in Nature that LHPP can also serve as a biomarker for the diagnosis and prognosis of liver cancer.
The incidence of liver cancer, also known as hepatocellular carcinoma, is steadily increasing. In the last twenty years, the number of cases has almost doubled in Switzerland. Hepatocellular carcinoma is usually diagnosed at a very late stage when the liver is already severely damaged and hence overall prognosis is poor. Detection of the anti-cancer protein LHPP as a biomarker may allow clinicians to provide better treatment options.
New anti-cancer protein LHPP
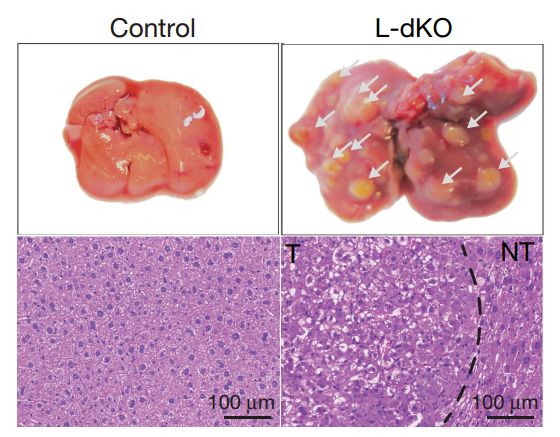
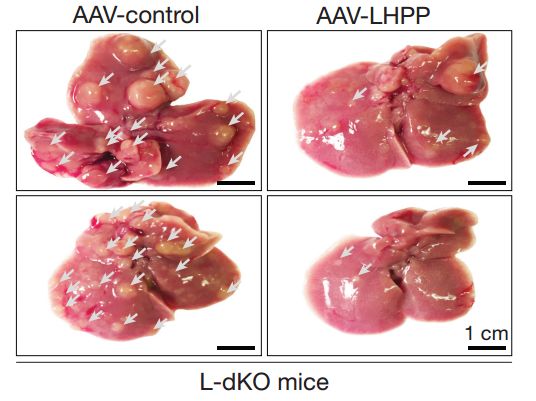
Liver tumors develop from mutated cells that grow and proliferate uncontrollably. Anti-cancer proteins, so-called tumor suppressors, prevent uncontrolled cell growth. Tumor suppressors are often defective in cancer cells. The researchers led by Prof. Michael N. Hall, Biozentrum of the University of Basel, have now discovered a new, so far unknown tumor suppressor, the protein LHPP. In their study, they show that the loss of LHPP promotes tumor growth and reduces the chance of survival of cancer patients. LHPP could potentially be used as a prognostic biomarker.
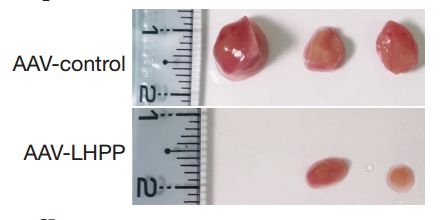
The researchers generated a mouse model for hepatocellular carcinoma by activating mTOR signaling specifically in the liver. They analyzed a total of more than 4,000 proteins, comparing them in healthy and tumor tissue. An enzyme emerged as the top favorite: the histidine phosphatase LHPP. "It is striking that LHPP is present in healthy tissue and completely absent in tumor tissue," says first author Sravanth Hindupur. Re-introduction of the genetic information for LHPP by the researchers prevents the formation of tumors and maintains liver function.
Loss of LHPP in cancer patients
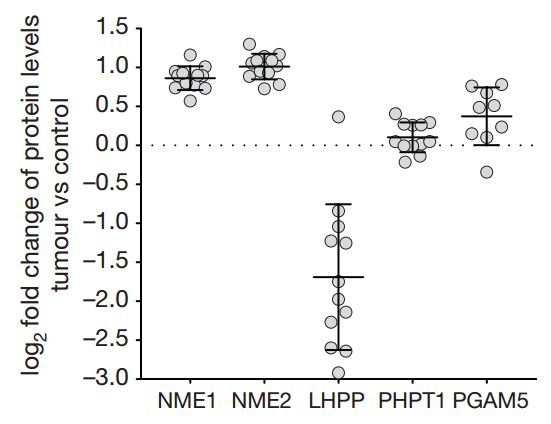
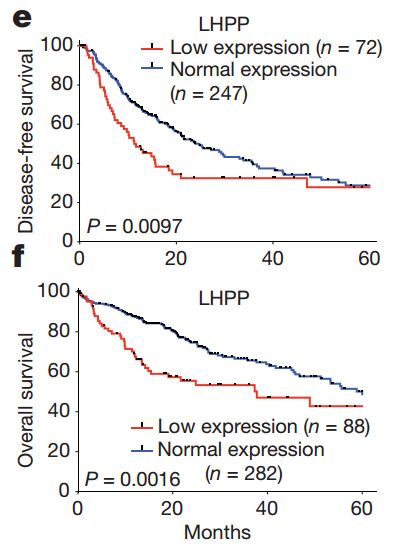
"Similar to the mouse model, we also saw a striking decrease in LHPP levels in tumors of patients with liver cancer," says Hindupur. Additionally, both disease severity and life expectancy correlate with LHPP levels. With complete loss of the tumor suppressor, cancer patients die on average two years earlier. LHPP is useful as a biomarker to classify tumors.
Phosphorylation important for tumorigenesis
LHPP is a phosphatase that removes histidine-linked phosphate groups from proteins. Like all amino acids, histidine is a basic component of proteins. Histidine phosphorylation of proteins has been poorly investigated due to the lack of suitable tools. "Tony Hunter, from the Salk Institute in the USA, has provided us with new tools to analyze histidine phosphorylation. We have now been able to visualize a whole new layer of complexity in tumor formation," says Hindupur.
Due to the absence of LHPP, global protein histidine phosphorylation is increased, which can lead to activation of several important functions and uncontrolled cell proliferation. This absence promotes the growth of tumors via increasing histidine-phosphorylated proteins. The tumor suppressor LHPP may also play a role in the development of other cancers.
More information: Sravanth K. Hindupur et al, The protein histidine phosphatase LHPP is a tumour suppressor, Nature (2018). DOI: 10.1038/nature26140











.jpg)
.jpg)
.jpg)
 香港港安腫瘤中心首席物理學家陳作良
香港港安腫瘤中心首席物理學家陳作良 設計治療計劃時,醫學物理學家會依據腫瘤的形狀、大小而制定放射治療的範圍和劑量。
設計治療計劃時,醫學物理學家會依據腫瘤的形狀、大小而制定放射治療的範圍和劑量。 電療設計必須一絲不苟,但同時也是一場與時間的競賽。Charlie表示,港安的電療服務可能是全港甚至全世界最快捷的。遇有特別情況,如病情需要,可安排翌日甚至即日進行電療。
電療設計必須一絲不苟,但同時也是一場與時間的競賽。Charlie表示,港安的電療服務可能是全港甚至全世界最快捷的。遇有特別情況,如病情需要,可安排翌日甚至即日進行電療。



.jpg)
.jpg)
.jpg)