










「推動香港中西醫結合治療肺癌交流研討會」第一天活動結束,感謝今天參加研討會的嘉賓、講者及參加者。 好榮幸能凝聚一眾具經驗的中西醫專家演講多個專業主題,深入交流有關肺癌臨床治療的最新技術、中西醫結合治療的最新進展及各種最新診斷方法。
最後,感謝各位同事及促成研討會的友好夥伴,期待明天的全新講者及分享!





更多花絮:
更多花絮:
癌症是本港的頭號殺手,而肺癌更是其中之首,2022年便有逾5,700宗新症,導致近3,800人死亡。幸而近年肺癌治療不斷突破,尤其是標靶治療及免疫治療等新式治療的出現,為肺癌病人帶來更多治療的希望,但要選擇合適及精準的治療方向不能靠估,而是需要利用次世代基因檢測等技術協助,幫助醫生和病人及早對「症」下藥,以獲得最大的治療效果。
臨床腫瘤科專科醫生蔡國強指出,與其他癌症一樣,肺癌能夠愈早發現,治癒機會也愈高,惟因為肺部體積大,又沒有痛覺受體,即使長有腫瘤也未必有症狀,直至入侵血管或骨骼才會出現較明顯徵狀,導致大部分病人確診時已屬較晚期。
早期肺癌可透過手術切除帶來根治的機會,或以立體定位放療消滅腫瘤,晚期肺癌則以藥物治療為主。過去晚期肺癌幾乎只有化療可用,但隨著醫學進步,化療已經不再是唯一或首選的治療,反而會透過檢測了解腫瘤基因特性,從而選擇最合適的治療。
蔡醫生直言,腫瘤基因檢測在晚期肺癌診治扮演重要的角色,原因現在很多新藥都是根據腫瘤特性而研發,能夠精準針對癌細胞的特點,讓醫生可以為病人度身訂造個人化的治療方案,帶來更理想及更顯著的治療效果。
要知道腫瘤特性,需要抽取病人的腫瘤組織或血液,再利用免疫組織化學染色法(Immunohistochemistry, IHC)、聚合酶連鎖反應(Polymerase Chain Reaction, PCR)PCR),以及近年面世的次世代基因排序(Next Generation Sequencing, NGS)等技術進行檢測。
蔡醫生稱,比起傳統技術,次世代基因排序的特點是敏感度高,且可以快速及一次過檢測多種基因特性,並能在不同的階段,幫助病人因應腫瘤變化配對合適藥物及預測治療效果,減少治療時走冤枉路的情況,譬如在確診時做檢測可以確定治療方向,當沿用治療失效後則可找出抗藥機制,以尋找其他更有效的治療。即使經過多線治療,仍有機會透過基因檢測確定是否有較罕見的基因突變。
事實上,市面有不同的NGS檢測套組(Panel),小套組涵蓋最常見且有相應治療可用的基因目標,大套組則包含更多及較罕見的基因項目,像與免疫治療相關的微衞星不穩定性(Microsatellite Instability, MSI)和腫瘤突變負荷(Tumor Mutational Burden, TMB);部分檢測套組會同時搭配不同檢測平台服務,提供PD-L1的表現狀況,及透過RNA定序找出相對較為少見的基因(融合)變異,以提供醫生及病人更完整的癌症分子檢測報告。
蔡醫生以一名年約六十歲的晚期肺癌病人為例,確診時檢測出見於近半數肺癌病人的EGFR (Epidermal Growth Factor Receptor)突變,於是使用相應的標靶藥,治療效果理想,病情受到良好控制。但約一年半後,病人的頸部長出新腫塊,檢測顯示除EGFR突變外,PD-L1(Programmed Death-Ligand 1)表達亦非常高,儘管EGFR突變型肺癌普遍對免疫治療效果不太理想,但根據檢測結果及臨床判斷,病人很大機會對免疫治療有反應,於是轉用免疫治療配合化療方案,結果病情得到顯著改善,三個月後頸部腫瘤更完全消失。
他指出,從上述個案的歷程表明基因檢測對於選擇合適的治療十分重要,因為若病人沒有檢測PD-L1,便可能無法受益於治療帶來的控病效果。由此可見,基因檢測能夠使醫生毋須「估估下」,可於最合適的時間選用最適合的治療,引導癌症治療邁向更精準及個人化,為病人帶來更多勝算。
對於不幸確診患上肺癌的病人,特別是晚期患者,蔡醫生寄語病人不要放棄,而親人朋友的鼓勵和同行,更是抗病過程中不可或缺的支持。他說,明白病人當刻可能會感到晴天霹靂,心情難免焦慮不安,甚至影響整個家庭,這時他會為病人清楚闡述病患的發展及治療,讓病人知道肺癌治療不斷出現多突破,存活的機會及時間都大為改善。

香港大學李嘉誠醫學院 (港大醫學院)研究團隊成功研發的三氧化二砷(俗稱砒霜)口服藥劑(藥用口服砒霜或ARSENOL®),可用於治療一種死亡率高的血癌 ── 急性早幼粒細胞白血病(acute promyelocytic leukaemia,APL)。藥用口服砒霜的發明和應用是香港醫學史上的重要里程碑,意義深遠。這不僅是香港首款自主發明和製造的處方藥,也是首個獲得美國、歐洲和日本專利的藥物。經過廿載的不懈努力,港大醫學院研究團隊成功轉化香港研發成果為臨床應用,將藥用口服砒霜納入APL患者的治療方案。過往廣泛的臨床研究結果顯示,藥用口服砒霜具有高效性和安全性,APL 患者的整體存活率超過97%,能顯著減輕副作用和治療負擔。
港大醫學院的研究團隊在藥用口服砒霜治療APL已進行超過20年的廣泛研究。在一項為期15年的前瞻性隨訪研究中,超過400名復發性APL患者接受以藥用口服砒霜為基礎的治療方案後,其分子生物學緩解率(molecular remission rate)和五年整體存活率分別高達100%和80%。這些成果是在未進行骨髓移植的情況下實現的;骨髓移植是一種高度有毒的治療方法,但全球多個沒有藥用口服砒霜藥劑的地區仍採用此方法。
隨後,研究團隊將藥用口服砒霜作為首次緩解後的維持治療,喜證五年無白血病存活率和整體存活率分別達至90%和97%。下一步是將藥用口服砒霜納入新確診APL患者的第一線誘導治療,並達至五年內100%無白血病的存活率和整體存活率。綜合目前的研究結果,港大醫學院的研究人員已制定一套治療計劃,重點包括及早開始治療、提供必要的支援性護理,以及在第一線誘導治療中使用藥用口服砒霜。這套治療計劃能有效減低APL併發症所引致的早期死亡率,過去這一比例可高達20%至30%。
研究團隊目前正在香港測試一種全口服治療方案(簡稱AAA),由藥用口服砒霜(Oral-ATO)、全反式維甲酸(all-trans retinoic acid,ATRA)及抗壞血酸(ascorbic acid)組成,並根據不同APL患者的風險進行調整。

這項研究的首席研究員、港大醫學院臨床醫學學院內科學系臨床副教授喬夏利醫生表示,這個全口服的治療方案非常有效和安全,能在專科門診環境下為不同風險水平的APL患者提供藥物治療,而不需要長期住院。藥用口服砒霜的治療方案可以大幅減少化療的使用,不僅適用於低風險的APL患者,而且適用於所有APL患者,包括兒童和成人。
作為將藥用口服砒霜推向國際醫療舞台的第一步,該藥已獲得美國食品及藥物管理局(FDA)及歐洲藥品管理局(EMA)的罕見病藥物資格認定(孤兒藥,orphan drug designation,ODD),亦同時取得美國 FDA新藥臨床研究資格認定(investigational new drug designation,IND)。這是首款由香港研發的抗癌處方藥物,獲得重要的FDA和EMA認證,對進行針對藥用口服砒霜的全球性研究至關重要。
APL 亞洲聯盟
由港大醫學院領導的APL亞洲聯盟 (APL Asian Consortium)由香港、馬來西亞、新加坡和台灣的研究人員組成,專注於APL的研究和治療。在其首個回顧性分析中,發現「AAA」較化療等傳統治療方案,更具優越性。APL 亞洲聯盟是目前在這些地區推廣藥用口服砒霜應用的重要平台,其在亞洲聯合進行的「AAA」研究項目獲港府創新及科技基金支持。
港大醫學院的研究人員與大灣區(通過香港大學深圳醫院)及亞洲地區(通過新加坡國立大學癌症中心及新加坡國立大學醫院)的研究人員攜手合作,推廣藥用口服砒霜的應用。該項跨中心研究顯示,三年整體存活率和無復發存活率分別為99%及97%。
此外,藥用口服砒霜亦獲得廣東省藥品監督管理局批准,經由香港大學深圳醫院在大灣區作臨床使用。在APL 亞洲聯盟的支持下,藥用口服砒霜亦可在新加坡、馬來西亞和台灣進行APL的研究及臨床之用。
英國的AML Research Network和卡地夫大學(Cardiff University)夥同港大醫學院科研人員合作,成功獲得英國血癌協會(Blood Cancer UK)資助,於英國境內進行第三期全國性研究,將藥用口服砒霜納入APL的前線醫療及護理;這標誌著香港醫藥發展的歷史性新里程。
美國和歐洲
美國FDA和EMA的罕見病藥物資格認定(ODD)為藥用口服砒霜的臨床研究提供了必要的監管要求。港大醫學院的研究人員將與業界合作夥伴攜手於今年在香港、北美及歐洲展開臨床研究計劃。
喬夏利醫生表示:「我們非常自豪能夠看到我們的研究成功轉化為臨床應用,惠及香港和世界各地病人。」他續說:「藥用口服砒霜的研發不僅為APL患者的治療方案帶來重大變革。這一便捷有效的治療選擇,能夠顯著改善患者的生活質素。對於能將這項創新研究成果推向世界並擔任先鋒角色,我們倍感自豪,並將致力於讓所有APL患者都能獲得這種挽救生命,且具有成本效益的療法。通過擴大藥用口服砒霜的普及性,我們期望APL成為可治癒的疾病,惠澤全球患者。作為醫生,這將是我們最大的心願和成就。」

發明:三氧化二砷口服藥劑(藥用口服砒霜或ARSENOL®)
發明者:港大醫學院臨床醫學學院內科學系榮休教授 Cyrus Kumana教授及講座教授鄺沃林教授
現時研究項目首席研究員:港大醫學院臨床醫學學院內科學系臨床副教授喬夏利醫生
研究項目由香港特區政府醫務衞生局醫療衞生研究基金資助,並獲創新及科技基金「夥伴研究計劃」資助。其他合作方包括香港大學技術轉移處和港大科橋有限公司(Versitech Ltd)、雅各臣藥業(Jacobson Pharma Corporation)、美國SDK Therapeutics Inc、新加坡國立大學癌症中心、新加坡國立大學醫院、英國AML Research Network、英國卡迪夫大學和英國血癌協會。

感恩癌症資訊網慈善基金被選中參與第二十六屆「 幸福的黃色小票 」活動。
AEON透過「幸福的黃色小票」,收集大家的祝福,轉化成捐獻送給社會各界有需要人士。
下週二 (2月11日 ) 「永旺日」,當天只要將在 AEON 購物後得到的黃色小票🏷 投放到寫有「癌症資訊網慈善基金」的投票箱🗳, AEON Stores Hong Kong 就會將收據金額的 1% 以捐助物品形式支持我們的癌症病人支援服務。 💪🏻
我們亦會於當天上午 11 時至下午6時於 AEON大窩口店 設置攤位,歡迎蒞臨參觀了解更多我們的服務,以及您如何可以參與其中。
Shopping and Blessings 【AEON x CICF 「幸福的黃色小票」🗳】
You can bless cancer survivors during the New Year! you can support Cancerinformation while purchasing festive items! Next Tuesday (11 February after shopping at AEON store, simply drop your yellow receipts into the designated “Cancerinformation.com.hk Charity Foundation” collection box, or vote online by AEON Mobile APP. AEON will donate goods equivalent to 1% of the total transaction amount to the Cancerinformation.com.hk Charity Foundation (CICF).
What is more, we will set up a promotional booth at the AEON Tai Wo Hau Store to raise public awareness of health. Hope you take this opportunity to learn about health information while you shop. Looking forward to seeing everyone there!
📍 AEON 大窩口店
荃灣荃華街3號悅來坊 B2-B3 號舖
下載AEON Mobile Apps 📱網上購物,亦請在應用程式內進行投票支持
癌症資訊網慈善基金
Cancerinformation.com.hk Charity Foundation
骨骼轉移是癌症其中一個最常見的擴散之一。腫瘤一旦生長在骨頭就會產生很多不同的併發症,例如是痛症、骨折、惡性高血鈣等。如果骨擴散是發生在脊椎骨上,更有機會因為腫瘤壓迫神經線而導致失禁、肢體麻痹、甚至癱瘓。一般而言,要治療擴散性癌症,除了透過藥物控制腫瘤外,醫生也會考慮配合放射治療,從而達致減少疼痛和減低骨轉移引發骨折或壓住神經的機會。
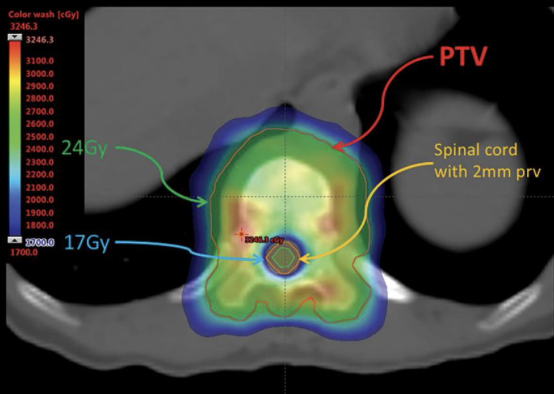
傳統電療有很多的局限性,例如在脊椎骨擴散,由於脊椎骨和脊髓神經很接近,高劑量電療有機會傷及脊椎神經,所以電療劑量會受到限制。同樣地,在治療其他骨擴散上,附近的正常器官,例如小腸、軟組織等,也會局限了電療的劑量。
近年,立體定位放射治療在骨擴散的應用已經十分普及。透過精準定位和影像導航,放射治療可以集中將高放射劑量準確投射到骨擴散上,提高對骨擴散的控制 ; 同時避免傷及旁邊的神經線或其他對放射電療劑量敏感的器官。研究顯示,透過立體定位放射治療以高劑量放射骨擴散,比傳統電療更有效改善痛症的控制和延長骨擴散無惡化存活期,減低骨轉移引起併發症的機會,提升病人生活質素。另外,有一些病人的骨擴散已接受過傳統電療,但因病情需要接受再度放射治療 (re-irradiation)。在此情況下,立體定位放射治療也有機會提高再度放射治療的電療劑量,增加骨擴散受控的機會。
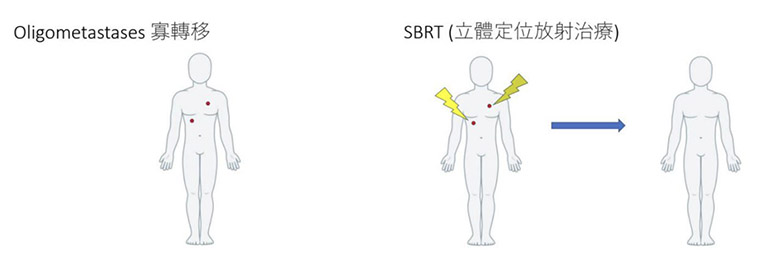
寡頭轉移(Oligometastases)是一個相對新的概念,指的是癌症細胞在身體的少數位置出現轉移,而非全身性散播。這種情況出現在某些癌症病患身上,如肺癌、前列腺癌、乳癌等。相比於全身轉移的情況,寡頭轉移患者的預後通常較佳,因此應積極尋求治療的機會。
寡頭轉移通常意味著腫瘤發生轉移的局部區域相對較小。與傳統的放射治療相比,SBRT能夠提供更高的輻射劑量,並將其準確地傳遞到轉移病灶周圍的組織中,以最大限度地減少正常組織的受損。 這種高度定位精度使得SBRT成為治療寡頭轉移的理想選擇。
SBRT在寡頭轉移的應用具有多個優勢。 首先,它能夠提供高劑量的輻射,以有效地控制和減緩轉移病灶的進展。 這對於控制寡頭轉移的生長和擴散非常重要,有助於延長患者的存活期。 其次,SBRT通常只需要幾個治療次數,每個電療持續時間較短,通常為幾分鐘到幾十分鐘。 相比於傳統電療的長期治療週期,SBRT為患者提供了更加方便和舒適的治療選擇。
在寡頭轉移的治療中,SBRT已經展現了良好的療效。許多研究顯示,SBRT能夠顯著延長寡頭轉移患者的無進展生存期和總生存期。對於多發性寡頭轉移,SBRT的作用也日益受到重視。一些研究表明,即使癌症已經轉移到多個部位,只要這些轉移灶數量有限(通常定義為1-5個)且可以全部用SBRT照射到,患者仍然能夠獲益。
此外,SBRT在寡頭轉移治療中的另一個重要作用,是可以與其他治療手段如手術、標靶療法、免疫療法等結合使用,發揮協同效應。這種聯合療法能夠進一步改善患者的治療效果和預後。例如,一些研究發現,對於某些轉移性前列腺癌患者,在行系統性藥物治療的同時,使用SBRT照射殘留的寡頭轉移灶,可以明顯延長無進展生存期。
除了以上優勢,SBRT還能夠有效地減輕患者的症狀和提高生活品質。 寡頭轉移往往會導致疼痛、壓迫或功能障礙等症狀,而SBRT可以通過減少腫瘤的負荷和壓迫,緩解這些症狀。 此外,由於SBRT的高精度和保護正常組織的能力,其治療副作用相對較小,患者的恢復時間也較短。
總的來說,SBRT已成為治療寡頭轉移的一種重要手段。其高精準性、高劑量和較少副作用的特點,使其在這一領域展現出不俗的治療效果。隨著技術的不斷進步和臨床研究的深入,SBRT在寡頭轉移治療中的地位必將進一步鞏固。需要注意的是,SBRT並非適用於所有寡頭轉移的患者。 治療決策應該是個體化的,並且應基於患者的整體健康情況、轉移病灶的位置和數量、以及其他相關因素進行綜合考量。患者應與主診醫生充分溝通,共同制定最佳的治療計劃。
未來,我們或許可以期待SBRT與其他治療手段的更多聯合應用,為寡頭轉移患者帶來更好的臨床結果。
![]()

🏃🏻個人簡介
Dr Wendy 黃韻婷博士 |香港註冊中醫師
🏅活動期望 / 心聲
忙到裙拉褲甩,我都會繼續陪你跑⋯⋯
唔係因為我得閒得滞無嘢做,因為為咗你,我講到做到!
2025年再次參加慈善跑10公里,係因為2024年我突破咗好多自己嘅安舒區!希望自己今年唔係興起,而是堅毅及身體力行,同你哋一齊持守向前行!
關於 渣打馬拉松2025馬拉松慈善計劃——醫患陪你跑
癌症資訊網慈善基金(CICF)很榮幸成為渣打馬拉松2025「馬拉松慈善計劃」的指定受惠機構之一 ,我們將派出「醫患陪你跑」隊伍參賽。「醫患陪你跑」隊伍由醫生和癌症病人組成,隊員將會結伴受訓,共同完成賽事,齊齊享受汗水所帶來的生命力和滿足感。
康復路程雖遠,我們會與您同行!
癌症資訊網慈善基金希望透過計劃宣揚互助互勉的健康正能量!
歡迎公眾捐款支持「醫患陪你跑」隊伍完成挑戰!
今年感謝港怡醫院團隊大力支持「醫患陪你跑」,籌得善款將用於「癌症病人復康支援服務」。
請各位關注癌症資訊網慈善基金社交平台,我們將會持續更新資訊!
#癌症資訊網慈善基金 #中西醫結合癌症
捐款Link:https://member.cancerinformation.com.hk/2024/12/渣打香港馬拉松2025「醫患陪你跑-」-黄韻婷博士

🏃🏻個人簡介
馬偉傑醫生 | 泌尿外科專科醫生
🏅活動期望 / 心聲
每一個落場跑的跑手,在起點時都未必清楚知道要轉多少個彎,上多少段斜,但肯定知道的就是只要沿著跑道向前跑,忘記背後,最終一定會到達終點,完成賽事。
今年我再次踏上跑道,以行動支持病患及家人一起面對癌症,努力向前。
關於 渣打馬拉松2025馬拉松慈善計劃——醫患陪你跑
癌症資訊網慈善基金(CICF)很榮幸成為渣打馬拉松2025「馬拉松慈善計劃」的指定受惠機構之一 ,我們將派出「醫患陪你跑」隊伍參賽。「醫患陪你跑」隊伍由醫生和癌症病人組成,隊員將會結伴受訓,共同完成賽事,齊齊享受汗水所帶來的生命力和滿足感。
康復路程雖遠,我們會與您同行!
癌症資訊網慈善基金希望透過計劃宣揚互助互勉的健康正能量!
歡迎公眾捐款支持「醫患陪你跑」隊伍完成挑戰!
今年感謝港怡醫院團隊大力支持「醫患陪你跑」,籌得善款將用於「癌症病人復康支援服務」。
請各位關注癌症資訊網慈善基金社交平台,我們將會持續更新資訊!
#癌症資訊網慈善基金 #醫患陪你跑 #同行向前
捐款Link:https://member.cancerinformation.com.hk/2024/12/渣打香港馬拉松2025「醫患陪你跑-」-馬偉傑醫生
顱內立體定位放射手術 (Stereotactic Radiosurgery, SRS) 可說是立體定位放射治療的鼻祖。這項技術由瑞典神經外科醫生Lars Leksell在1950至60年代發明,旨在利用高劑量輻射,針對腦部細小目標進行非常精確的放射治療。顱內立體定位放射手術 SRS 是一次性的放射治療,有如手術 (Surgery) 一次便可以完成;若需要多於一次的治療,則稱為顱內立體定位放射治療 (Fractionated Stereotactic Radiotherapy, FSRT)。
適用於腦轉移 (brain metastasis) 控制,也可用於其他良性情況,例如聽覺神經瘤(acoustic neuroma)、動靜脈血管畸形瘤(arteriovenous malformation)、 腦膜瘤 (meningioma) 等。
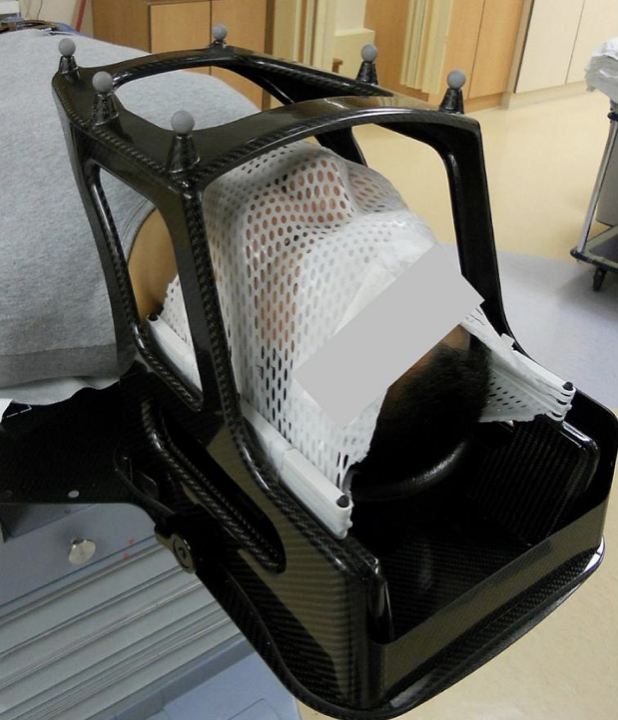
SRS 或者 FSRT 治療次數一般只有一次至五次不等,治療精準度亦相當高。為了保持治療必須的精準度,定位的步驟非常重要。傳統的方法是由神經外科醫生為病人以局部麻醉的方式裝上定位框架 (stereotactic frame),再利用三維立體定位技術確定目標位置作 SRS 或 FSRT 治療。配戴定位框架的時間長達6-7小時,對病人來說並不舒適。隨着放射科技的發展,現代的SRS 和 FSRT治療利用更先進的儀器和立體定位技術,不再需要用到入侵性的框架,而可用無框頭模治療 (frameless SRS or FSRT),這既能確保治療的準確度和效率,也能大大提高病人的舒適度和對於治療的配合。
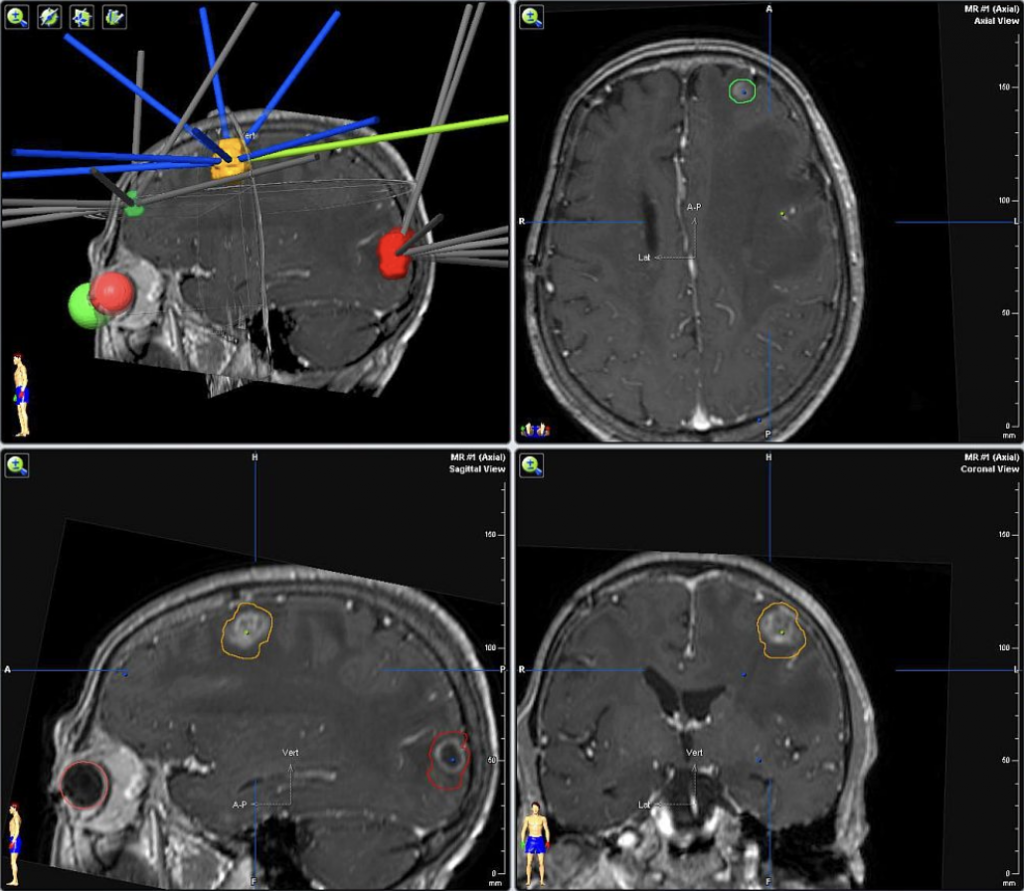
現在,一般的 SRS 和 FSRT 都以直線加速器 (Linear Accelerator) 配以高解像度的多葉準直儀 (multileaf collimator, MLC) 進行,也有以更精準的伽碼刀 (Gamma knife)、數碼導航刀(Cyberknife) 進行。由於治療的複雜度高,所以實在需要臨床腫瘤科醫生、神經外科醫生、醫學物理學家及放射治療師等醫護人員合作,制定病人的 SRS 或 FSRT 的治療計劃。在醫生規劃好治療目標和範圍之後,醫學物理學家和放射治療師會使用立體定位系統,為病人制定非共平面 (non-coplanar) 的強度調控放射治療 (intensity-modulated radiotherapy, IMRT) 或弧形調控放射治療 (volumetric modulated arc therapy, VMAT) ,以達致高能量放射線的治療安排。治療團隊亦會視乎病灶的分佈來決定靶區的數目,每個靶區的治療時間約為20-30分鐘不等。各間醫院也逐漸引入新型技術,以至一次可以對準大概不多於10個腦轉移,大大縮減治療時間。
為了配合高精準度的治療,對位校正亦需要用到先進的實時影像導航技術 (real-time image guidance),例如有X光感測器、紅外線影像導引的功能設備,加上六維移動的治療床 (6D treatment couch) 的配合,打造出少於1毫米的精確度。若腫瘤位置在治療期間出現偏差,系統會顯示訊息,放射治療師便需要暫停治療,移動治療床作重新對位後,才可以再繼續治療。
隨着抗癌治療的進步和腦部掃描的普及化,晚期癌症病人發現腦轉移的時候,原發的癌症 (例如比較常見的有肺癌和乳癌) 在顱外往往仍有不錯的整體控制,而病者本人的狀態仍然良好。SRS 和 FSRT 的治療技術,可以容許以無創的方式,針對性地治療一粒甚至多粒的腦轉移,達致縮小、甚至消除病灶的效果。
基於其高精準度,這治療方法相比傳統的全腦放射治療 (Whole Brain Radiotherapy, WBRT),更能避免或減少對於顱內正常結構組織 (例如腦幹、視覺神經中樞、海馬體等等) 的輻射,減少腦部認知因為治療而受影響的程度。
而且,透過非入侵性的無框頭模治療,病人可避免接受開腦手術的種種風險,而可得到有如開放性外科手術般有效的治療成功率。
SRS 或者 FSRT 亦有其副作用,病人可能會有頭痛、暈眩、疲倦、嘔心的症狀。在治療範圍的皮膚可能有刺激性發炎、或有局部脫髮的狀況。神經系統徵狀也有可能出現,例如抽搐、麻痺。經醫生處方類固醇或其他紓緩症狀的藥物,一般都會有所改善。
整體來說,顱內立體定位放射電療技術已經相對成熟,病人副作用大大減少,而成效也顯著。然而每位病人的情況都不一樣,建議向專科醫生索取更多資訊。
![]()

隨着內地與香港交流愈趨頻繁,兩地醫療逐步接軌,港人跨境就醫需求日增。香港 青年協會青年研究中心成立的「青年創研庫」12月8日公布「優化跨境就醫應對 醫療需求」研究報告。結果顯示,在600名受訪的香港市民中,超過七成六(76.3%) 認同跨境就醫有助增加醫療選擇,並且近七成(69.5%)認同有助紓緩公營醫療壓 力。
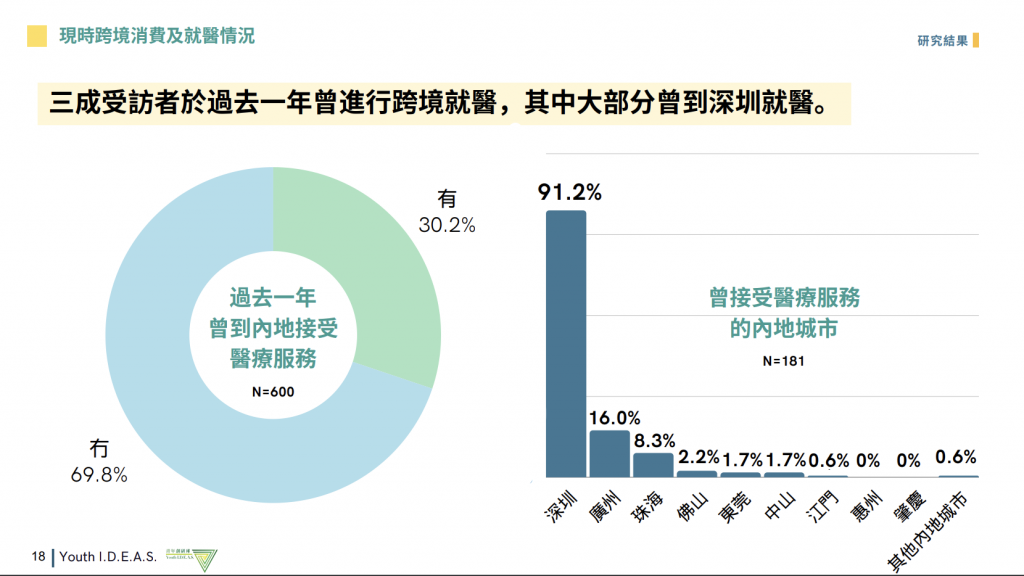
調查顯示,三成(30.2%)受訪者於過去一年曾赴內地就醫【表3】,當中大部分(91.2%) 選擇深圳【表4】,主要進行牙科檢查(66.3%)和身體檢查(29.8%)【表5】。促 使他們選擇內地就醫的主因包括「醫療費用較低」(85.1%)和「輪候時間較快」 (49.7%)等。
此外,七成(69.8%)未曾使用內地醫療服務的受訪者,主要原因是「對內地醫療 不認識」(51.3%)和「擔憂醫療質素」(34.8%)等。

調查結果顯示,受訪者對跨境就醫有潛在顧慮,包括「內地各醫療機構設備標準不 一,質素參差」(54.5%)、「兩地醫護人員資歷認證不同」(34.0%),以及「醫 療事故的賠償及權責問題」(33.0%);另外,他們亦對「兩地相關法規和規管制 度不同」(24.7%)、「內地醫療報告不獲港醫接納」(13.5%),以及「資訊透明 度不足」(12.8%)等感到擔憂。
上述研究於今年10月至11月期間,以實地意見調查訪問了600名18至74歲香港居民, 同時亦訪問了18名個案。研究發現,逾八成三(83.3%)同意對內地醫療不了解【表 9】;整體而言,他們對內地醫療的信心一般,平均分為5.02(0-10分,10為最高)。

相比之下,受訪者對本港醫療體系予以肯定。絕大部分(99.0%)對本港醫療體系 表示信任【表12】,整體平均分高達7.96(0-10分,10為最高)。
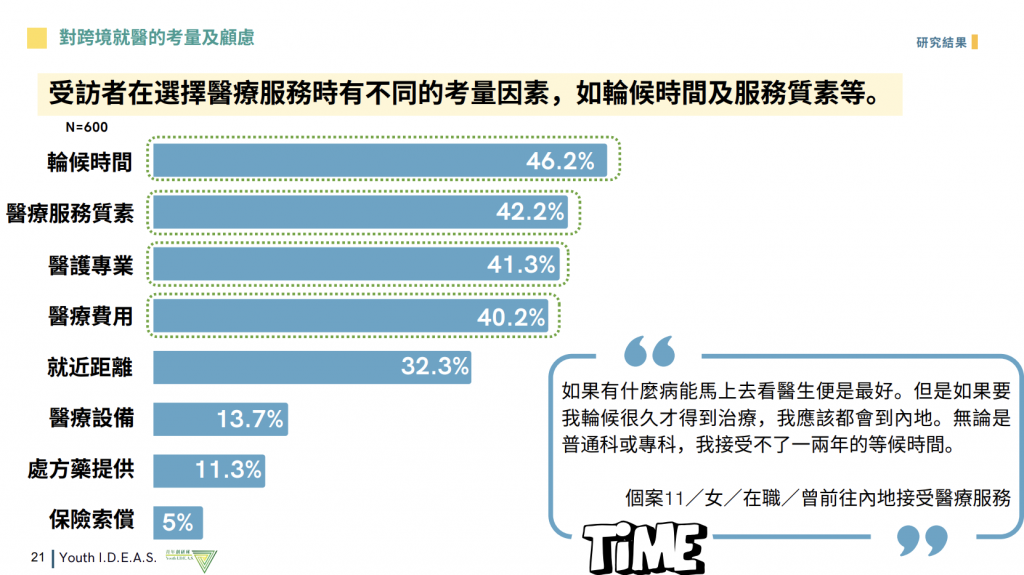
在選擇醫療服務時,受訪者的主要考慮因素依次為輪候時間(46.2%)、服務質素 (42.2%)、醫護專業(41.3%)及醫療費用(40.2%)。
綜合個案訪問意見,有個案提到內地醫療費用相對便宜,但缺乏接收資訊的渠道, 只靠親友口傳介紹;有個案坦言對內地醫療不甚了解,以致信心不足。 2024 年 12 月 8 日 新 聞 稿 2 / 2 研究亦訪問了5位熟悉有關議題的專家。有受訪專家對關注兩地的醫學語言術語及 表達方式存在差異,報告用詞或會引起醫療判斷偏差;另有專家指出內地的法規制 度及事故處理方法與香港不同,建議市民赴內地就醫前應主動了解相關制度及投訴 機制,以保障自身權益。
青年創研庫社會民生組召集人倪智承指出,現時跨境就醫仍是起步階段,需進一步 促進兩地醫療合作及溝通。他引述研究報告指,建議當局成立「粵港跨境醫療專責 小組」,統籌香港與大灣區的跨境醫療事務,主要職能包括:設立專門的投訴渠道、 制定公共衞生應急方案,以及促進兩地醫療信息共享及專家交流。
該組副召集人郭達生指出,因應港人對內地醫療的了解不足,建議設立一個透明且 方便使用的資訊平台,發布跨境醫療的最新政策措施及內地醫療相關服務資訊,確 保資訊準確及一致,並結合地圖及定位功能,提供內地三級甲等醫院的名單和地理 位置,方便市民查詢。
為有效彌合兩地醫學術語的差異,該組成員程智楓認為兩地院校應合作建立語料庫 (Corpus),整合兩地的醫學術語,並同步提升「醫健通」功能,讓上傳的跨境醫 療報告能應用語言支援。他亦建議加快優化長者醫療券計劃,逐步覆蓋更多服務試 點,以回應香港長者的殷切需求。
有關青年創研庫 青協青年研究中心自2015年起成立「青年創研庫」,是本港一個屬於青年的智庫。 現屆(2023-2025年度)創研庫成員由近80位本地青年專業人士與大專學生組成, 平均年齡為27歲。透過以研究實證為基礎的討論、交流,創研庫成員提出政策建議, 期望能為社會建言獻策。青年創研庫三項專題研究系列包括:「經濟就業」、「青 年發展」,以及「社會民生」。5位專家、學者應邀擔任創研庫的顧問導師,包括張 子欣博士、倪以理先生、張炳良教授、陳智遠先生,以及范寧醫生。
「伴你同行日」步行活動於2024年12月14日舉行,活動由香港大學臨床腫瘤學系「家支援」及癌症資訊網慈善基金合辦,聯同六大與癌症有關的慈善機構協辦,包括粉紅社、全球華人乳癌聯盟、同路人同盟、GistUnion 和香港肝臟移植協康會。




「伴你同行日」步行活動共有近三百名癌症病友和照顧者參加。「家支援」項目負責人香港大學臨床腫瘤學系陳穎樂醫生指出活動目標是鼓勵癌症病友和家人能多做運動,鍛鍊體能。美國運動協會建議,癌症病友無論是治療當中或治療完畢,每星期做150分鐘中強度或70分鐘高強度運動。主辦機構選擇在中山紀念公園行至金紫荊廣場,在鬧市中找一路段,行45至60分鐘。日行10,000步,由中山紀念公園行至金紫荊廣場,大約6500步,運動應由基本做起,步行不需要有任何工具,簡單又容易。而且也鼓勵參加者以小組形式參加,在這癌症路上,總會有很多高低起跌,若有人同行,必定輕鬆很多。也感謝中國銀行(香港)全額資助家支援應用程式。
癌症資訊網創辦人吳偉麟也是癌症復康者,也曾經歷過艱辛的治療旅程,指出社區上有不同的癌症病人組織,大家互相聯合一同為癌症病友服務,令癌症病友在這抗癌路上不孤單。




步行日也邀請了兩位癌症康復者,粉紅社創辦人關裕穠女士(關姐姐),於2008年確診第三期乳癌,經歷過化療、電療和荷爾蒙治療,感到腋下淋巴位置疼痛,於是開始學習伸展運動來幫紓緩痛症。後來關姐姐更成為伸展導師和彈力帶導師,教導乳癌康復者做毛巾操,因毛巾操能改善繃緊和紓緩手腫。關姐姐也在步行前和參加者一同做毛巾操,教大家做手部和腳部拉筋訓練。另外,梁玉玲師傅是一位胃癌康復者,她是中國香港健身總會導師。活動中,梁師傅與學生帶領參加者一起做簡單八段錦,八段錦總共有八招,是一靜一動的身心靈運動,就好像人生哲學「一鬆一緊」,有時候需要放鬆,不能繃得太緊;但太過放鬆,又會失去控制,需要從中取得平衡。

開步禮結束後,參加者一同由中山公園行至金紫荊廣場,天氣雖然有點寒冷,但陽光普照,而且參加者心內都很火熱,一面行,一面在海濱長廊打卡,留下開心愉快的回憶。
