醫療新知 >
【世界肺癌大會】Brief Report: Real-World First Round Results from a Charity Lung Cancer Screening Program in East Asia
【世界肺癌大會】Brief Report: Real-World First Round Results from a Charity Lung Cancer Screening Program in East Asia
11-09-2024
Brief Report: Real-World First Round Results from a Charity Lung Cancer Screening Program in East Asia
Alan D. L. Sihoe, MBBChir, FRCSEd,1, 2* Natalie K. Y. Fong,3 Alex S. M. Yam,3 Maria M. W. Cheng,3 Dorothy L. S. Yau,3 Alan W. L. Ng3
1CUHK Medical Centre, Hong Kong SAR, China. 2Gleneagles Hong Kong Hospital, Hong Kong SAR, China. 3Cancer Information Charity Foundation, Hong Kong SAR, China. * Corresponding author
Disclosures:
The charity screening program – but not this retrospective study – was partly sponsored by a charitable donation to the charity from Medtronic (Minneapolis, MN, USA) via Medtronic Hong Kong Medical Ltd.
Dr Sihoe reported receiving consulting fees or honoraria from AstraZeneca, Roche, Medela and Medtronic outside of the submitted work; and having leadership roles in the Asian Society for CardioVascular and Thoracic Surgery, the Asia Thoracoscopic Surgery Education Platform and the Society of Thoracic Surgeons. The remaining authors declare no conflict of interest.
Abstract
Introduction
Screening with Low Dose Computed Tomography (LDCT) has been proven to potentially reduce the rate of mortality of lung cancer. Lack of real-world data outside of protocolized trials has been cited as an impediment to its more widespread implementation, especially in Asia.
LDCT consultation section by Dr. Alan Sihoe
Methods
A single round of LDCT was provided through a community-based charity program in Hong Kong to asymptomatic adults with a family history of lung cancer and/or smoking history. Anonymized data from this program was analyzed.
Results
LDCT was performed for 99 participants, including 98 (99%) who had one or more family members with history of lung cancer, and 70 (71%) who were never-smokers. After a single round of screening, a positive LDCT was noted in 47 participants (47%). A sister with a history of lung cancer (28% versus 8%, p = 0.01) and a multiplex family (47% versus 23%, p = 0.02) were factors associated with a positive LDCT. Lung cancer (all adenocarcinoma) was diagnosed as a direct consequence of positive LDCT findings in 6 participants (6%), of whom 4 had stage I disease and 5 received surgery with curative intent. In the 47 participants with a positive LDCT, having a sister with a history of lung cancer increased the risk of a lung cancer diagnosis (relative risk = 5.23, 95% confidence interval: 1.09 – 25.21). Detected lesions categorized as Lung-RADS 3 or above (odds ratio = 12.08, 95% confidence interval: 1.27 – 114.64) or deemed by an experienced specialist to be suspicious (odds ratio = 63.33, 95% confidence interval: 5.48 – 732.29) were significantly more likely to turn out to be a lung cancer.
Conclusions
This real-world data demonstrates that a single round of LDCT screening at a community level in East Asia can detect potentially curable lung cancer at a rate comparable to those reported by protocolized trials. When considering future LDCT screening programs in East Asia, a family history of lung cancer may be a key factor indicating a person for screening, and how features of a LDCT-detected lesion should trigger further intervention warrant further definition.
Introduction
Screening with Low Dose Computed Tomography (LDCT) has emerged as potentially the most powerful means of reducing the mortality of lung cancer [1-3]. The American National Lung Screening Trial (NLST), the European NELSON trial, and the TALENT study from Taiwan demonstrated that LDCT can detect early stage lung cancer, potentially allowing curative therapy [2-4].
However, the implementation of LDCT screening worldwide has encountered resistance [5-6]. This has been attributed to a lack of: real-world data outside of clinical trials; global consensus over risk factors identifying eligibility for screening; understanding of how screening-detected lesions are managed in real-world healthcare systems; and so on. In particular, the results of clinical trials may have been obtained in highly selected cohorts, following specific protocols, predominantly at large academic institutions [7-9]. There is growing recognition that more real-world data is required to help the formulation of future lung cancer screening algorithms.
This study aims to analyze the data collected from the first round of a community-based, charity LDCT lung cancer screening program in Hong Kong to understand whether the efficacy of LDCT screening seen in international trials can be replicated in a real-world setting.
Patients and Methods
Patients and Management
From December 2021 to November 2022, a Charity Foundation in Hong Kong offered a single round of free LDCT screening to 100 eligible applicants from the public on a ‘first come, first served’ basis. Participation was voluntary and no incentives were offered to participants. The eligibility criteria were: asymptomatic; age 40 years or older; smoking history and/or family history of lung cancer; no history of previous malignant disease within the past 10 years; and ability to provide informed consent.
Each LDCT scan was assessed by the reporting radiologist, and separately by a specialist surgical oncologist with over 20 years’ experience in treating lung cancer. A LDCT scan was defined as positive if both the reporting radiologist and the specialist noted one or more discrete non-calcified lung nodular lesion. Each lesion was classified as a solid nodule, part-solid nodule, or ground glass opacity (GGO), and further categorized using the Lung-RADS™ Version 2022 Assessment [10]. The specialist additionally gave a comment on whether any identified lesion appeared suspicious of being a malignant neoplasm, and warranted further medical attention. As the charity was not a medical facility, any such further medical management was undertaken by the public health service of Hong Kong.
The charity subsequently maintained phone contact with all screening program participants. Participants were invited to report (on a voluntary, non-incentivized basis) if they were subsequently diagnosed to have lung cancer.
Data Collection and Analysis
This was a retrospective observational study analyzing previously collected data from a single participant cohort.
The data collected by the charity during the screening program were anonymized prior to analysis. All participants were contacted by the charity and all confirmed their consent for their anonymized data to be used in this study. The study was conducted in accordance with the 1996 Declaration of Helsinki, and was approved by the Ethics Committee of the Hong Kong Doctors Union.
The primary end point was the rate of detection of any biopsy-confirmed lung cancer. Fisher’s exact test or two-sample t test was used to test the difference between groups for categorical data or continuous data, respectively. All statistical tests were performed using MedCalc® Statistical Software version 22.017 (MedCalc Software Ltd, Ostend, Belgium).
Results
Participants’ Demographic and Clinical Characteristics
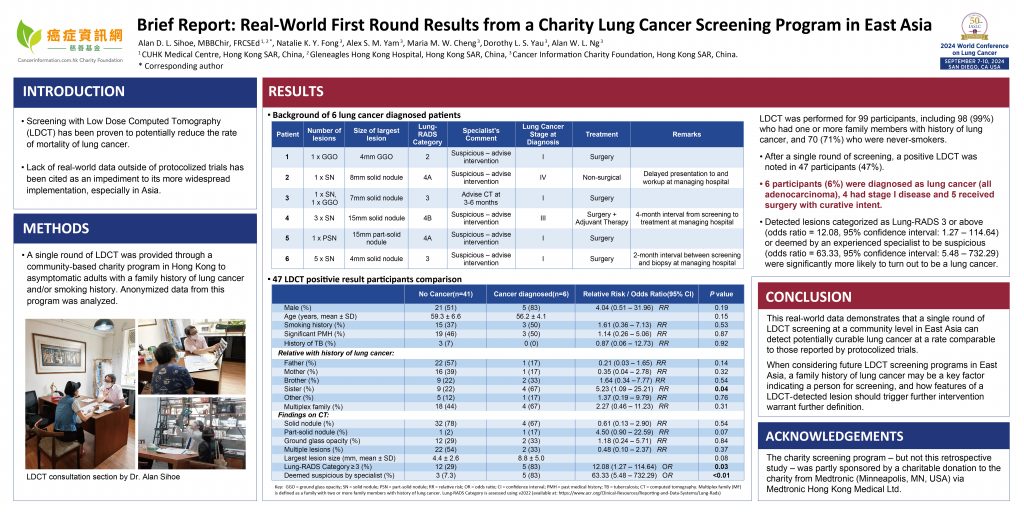
One LDCT scan was arranged for each of 100 participants meeting the eligibility criteria, but one participant withdrew before the LDCT was performed. Data for the 99 participants who received LDCT were analyzed, and their demographic and clinical characteristics are summarized in Table 1. A history of lung cancer in one or more family members was reported by 98 participants (99%). There were 45 participants (45%) who come from a multiplex family (MF), defined as a family with two or more family members with history of lung cancer. There were 29 participants (29%) with a history of smoking, including 16 current active smokers (16%), and 13 ex-smokers (13%).There were 45 participants (45%) with a significant past medical history, defined as having had previous major surgery/intervention or current medical therapy for any non-traumatic pathology.
Table 1:Demographic and clinical characteristics for the 99 participants who received LDCT
Key: CT = computed tomography; SD = standard deviation; PMH = past medical history; TB = tuberculosis
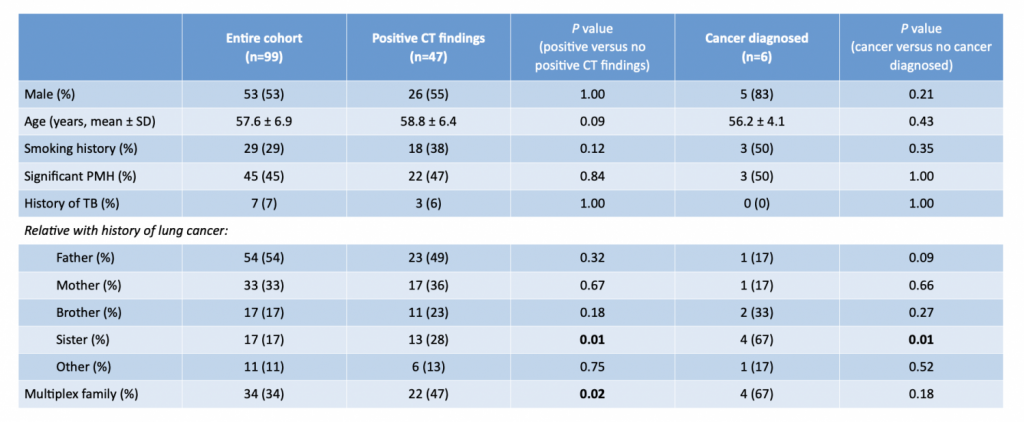
Table 2:Background of 6 lung cancer diagnosed patients
After this single round of screening, a positive LDCT was noted in 47 participants (47%). Multiple (more than one) lesions on LDCT were noted in 24 participants (24%). At least one solid nodule, part-solid nodule, or ground glass opacity (GGO) was found in 36 (36%), 2 (2%), and 13 (13%) participants respectively. A sister who had lung cancer and a multiplex family were factors associated with a positive LDCT (Table 1).
Of the 47 participants with a positive LDCT, the largest lesion was Lung-RADS category 3 in 12 participants (12%) and Lung-RADS 4 in 5 participants (5%).
The experienced lung cancer specialist commented that the identified lesions in 8 participants (8%) were suspicious of being malignant, and advised intervention. These 8 lesions included Lung-RADS category 2, 3 and 4 lesions in 2, 2, and 4 participants respectively. When correlating the specialist’s comment of a suspicious lesion with a Lung-RADS category of 3 or more, the inter-observer agreement test Weighted Kappa value was 0.40, indicating fair agreement.
Lung Cancer Incidence and Outcomes
After this single round of LDCT screening, a biopsy-confirmed diagnosis of lung cancer was made in 6 participants (6%). In all 6 participants, the diagnosis was a direct consequence of investigations pursued for positive LDCT findings from the screening. In all 6, the histological type was adenocarcinoma. The characteristics of these 6 participants are summarized in Tables 1 and 2.
One patient had stage IV disease by the time of diagnosis and received palliative therapy only. The other 5 participants diagnosed with lung cancer (83%) received surgery with curative intent. Four of those with lung cancer (67%) had stage I disease. In the 2 participants with stage III and stage IV disease, there was a substantial time interval (reportedly 2-4 months) between the LDCT being done and the diagnosis being eventually obtained.
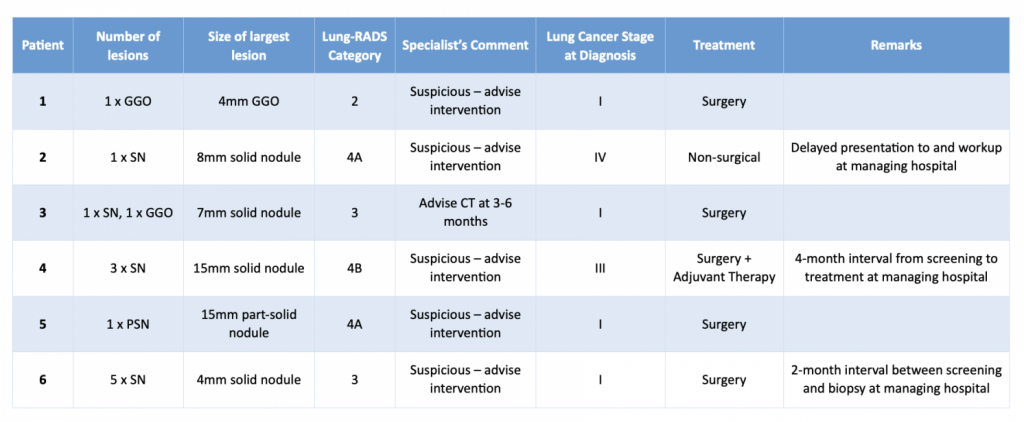
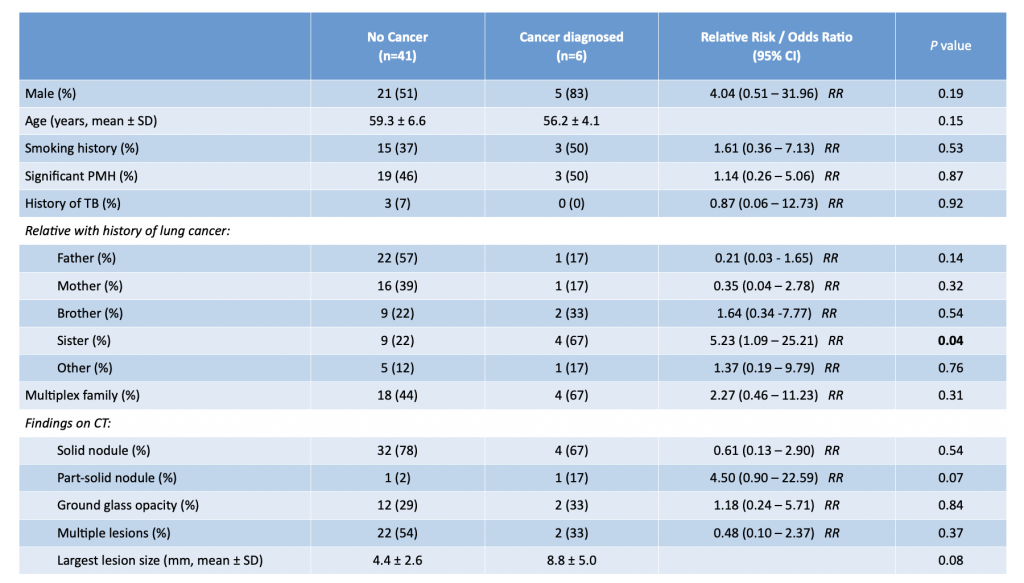
Table3: 47 LDCT positivie result participants comparison
Key: RR = relative risk; OR = odds ratio; CI = confidence interval; PMH = past medical history; TB = tuberculosis; CT = computed tomography Multiplex family (MF) is defined as a family with two or more family members with history of lung cancer. Lung-RADS Category is assessed using v2022 (available at: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Lung-Rads)
Table 3 summarizes the risk factors analyses for lung cancer amongst the 47 participants with positive LDCT. Having a sister with a history of lung cancer was the only identified patient factor predictive of lung cancer (relative risk = 5.23, 95% confidence interval: 1.09 – 25.21, p = 0.04). Both a Lung-RADS category of 3 or above and a specialist’s comment of a suspicious lesion were significantly predictive of a positive LDCT lesion turning out to be a lung cancer. Five (83%) of the 6 patients with lung cancer had a Lung-RADS 3 or above lesion, compared with 12 (29%) of the 41 positive LDCT patients not reporting cancer (odds ratio = 12.08, 95% confidence interval: 1.27 – 114.64, p = 0.03). Five (83%) of the 6 patients with lung cancer had a lesion deemed suspicious by the specialist, compared with 3 (7.3%) in the 41 LDCT positive patients not reporting cancer (odds ratio = 63.33, 95% confidence interval: 5.48 – 732.29, p < 0.01).
In addition, a seventh participant was subsequently found to have stage I lung cancer despite not having positive findings on the first round of LDCT. Because of his raised awareness of the importance of screening, he later sought out a follow-up LDCT at an undisclosed time later. This follow-up scan detected lung cancer for which he received surgery with curative intent.
Discussion
After a single round of community-based, charity-provided LDCT lung cancer in Hong Kong, 6% of participants were found to have lung cancer, of whom 83% received curative intent surgery. In comparison, the NLST and NELSON trials reported lung cancer detection rates of 4% and % respectively, but only faster multiple rounds of LDCT [2, 3]. The TALENT study from Taiwan detected 311 lung cancers (3%) among 12011 participants after a single round of LDCT screening [4]. Rates of diagnosis of lung cancer after only the first round of screening in the NLST and NELON trials were 1.1% and 0.9% respectively [2, 3]. Single round detection rates of 0.5-1.5% have previously been reported in studies from the USA and China [11-13]. Our results suggest that LDCT can be potentially effective in a real-world setting outside of clinical trials or health authority-provided programs, even with a single round offered. The seventh patient diagnosed with lung cancer after he pursued a follow-up LDCT himself after a negative first LDCT suggests that the raising of awareness from a single round may provide potentially lasting health education benefits.
Identification of a “high risk” population to screen is a key consideration for planning LDCT screening programs [6, 9]. Hitherto, prominent guidelines tended to focus on age (typically 50 years or older) and a long smoking history (typically ≥20 pack.years) as the primary selection criteria [14, 15]. However, recent evidence suggests that if such criteria were applied in an East Asian population, a majority of lung cancer cases may be missed [16]. The TALENT study targeted non-smoking persons in East Asia and found equal or greater lung cancer detection rates than Western screening studies focused on smokers [4]. These findings suggest that smoking should perhaps play a lesser role in Asia [5, 17]. Instead, a follow-on to the TALENT study demonstrated that a family history of lung cancer (especially maternal relative history) may be an even stronger risk factor in East Asian non-smokers [18]. The cohort in our screening program included 99% of participants having a family history of lung cancer and only 29% who were current- or ex-smokers, supporting family history may be more important than smoking as a selection criterion. If the NLST criteria had been applied in our screening program, 3 of the 6 cases of lung cancer (50%) would have been denied screening because they were never-smokers.
Another concern with LDCT screening is potential “over-diagnosis” due to “unnecessary” interventions for benign/indolent lesions [19-21]. Proposals to select only “high risk” lesions for intervention have included: Lung-RADS categorization; volumetric or AI analysis; supplementary liquid biopsy molecular testing; and others [6, 10, 22-24]. Most of these are insufficiently mature for clinical use, though Lung-RADS categorization is gaining widespread acceptance [10]. In our screening program, a Lung-RADS category of 3 or higher was associated with a diagnosis of lung cancer, but only 5 of the 17 participants (29%) with a Lung-RADS 3 or higher lesion were found to have lung cancer, suggesting suboptimal specificity. Instead, suspicious of malignancy by an experienced lung cancer specialist appeared to be even better correlated with lung cancer. The expertise of an individual specialist cannot be used as the basis to plan future screening programs, but our results suggest that more reliable means of selecting lesions for intervention than the current Lung-RADS system may exist.
To be effective at reducing mortality with screening, the interval from detection on LDCT to diagnosis or treatment is potentially critical [25, 26]. In our cohort, one participant had stage IV disease at the time of diagnosis, and another had stage III disease. In both cases, a significant interval (over 2 months) was noted between detection on screening and management by the public health service. Future screening programs should consider a mechanism for expeditious handover from the screening unit to the intervention unit in order to realize the maximal potential of screening to reduce mortality.
This report does have limitations. As this was not a formal trial, there was no mechanism for follow-up of participants. Hence, the outcomes of those 93 participants not reporting lung cancer are not fully known, even though some had lesions categorized as Lung-RADS 3 or greater. Also, since no true negative figure is available, accuracy results for LDCT cannot be computed. It is also acknowledged that our cohort was limited by the charity budget, and was small compared to those in previous major trials of LDCT screening. However, our data nevertheless provide one of the first real-world representations of LDCT screening in a community outside the highly-selected cohorts of an academic trial or government registry.
The experience of this community-based charity lung cancer screening project demonstrates that first round LDCT screening can provide real-world lung cancer detection results equivalent to or better than those achieved through highly selective and protocolized clinical studies. The results also suggest that different selection criteria for screening may exist in different populations (such as family history in East Asian populations), and that an optimal management pathway for screening-detected lesions remains to be defined.
Credit Authorship Contribution Statement
Alan D. L. Sihoe:Conceptualization, Formal analysis, Investigation, Methodology, Writing—original draft preparation, Writing—reviewing and editing.
Natalie K. Y. Fong: Data curation, Validation, Investigation, Writing—review and editing.
Alex S. M. Yam, Maria M. W. Cheng, Dorothy L. S. Yau, Alan W. L. Ng: Data curation, Investigation, Writing—review and editing.
References
Yu SWY, Leung CS, Tsz CH, Lee BTY, Chan HK, Sihoe ADL. Does low-dose computed tomography screening improve lung cancer-related outcomes? – a systematic review. Video-assist Thorac Surg 2020; 5:7.
National Lung Screening Trial Research Team, Aberle DR, Adams AM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365:395-409.
de Koning HJ, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N Engl J Med 2020; 382:503-513.
Yang P. National Lung Cancer Screening Program in Taiwan: The TALENT Study. J Thor Oncol 2021; 16:S58.
Osarogiagbon RU, Yang PC, Sequist LV. Expanding the Reach and Grasp of Lung Cancer Screening. Am Soc Clin Oncol Educ Book 2023; 43: 1-13.
Lam S, Bai C, Baldwin DR, et al. Current and Future Perspectives on Computed Tomography Screening for Lung Cancer: A Roadmap From 2023 to 2027 From the International Association for the Study of Lung Cancer. J Thorac Oncol 2024; 19: 36-51.
Chodankar D. Introduction to real-world evidence studies. Perspect Clin Res 2021; 12:171-4.
Liu F, Demosthenes P. Real‑world data: a brief review of the methods, applications, challenges and opportunities. BMC Medical Research Methodology 2022; 22:287.
Optican RJ, Chiles C. Implementing lung cancer screening in the real world: opportunity, challenges and solutions. Transl Lung Cancer Res 2015; 4:353-364.
American College of Radiology. Lung-RADS® v2022. Available at: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Lung-Rads (accessed on: 24 Jan 2024)
Kinsinger LS, Anderson C, Kim J, et al. Implementation of Lung Cancer Screening in the Veterans Health Administration. JAMA Intern Med 2017; 177:399-406.
Fan L, Wang Y, Zhou Y, et al. Lung Cancer Screening with Low-Dose CT: Baseline Screening Results in Shanghai. Acad Radiol 2019; 26:1283-1291.
Li Y, Du Y, Huang Y, et al. Community-based lung cancer screening by low-dose computed tomography in China: First round results and a meta-analysis. Eur J Radiol 2021; 144:109988.
Wolf AMD, Oeffinger KC, Shih TY, et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA Cancer J Clin 2024; 74:50-81.
National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Non-Small Cell Lung Cancer Version 2.2024. Available at: https://www.nccn.org/guidelines/category_2 (accessed on: 24 Jan 2024)
Qian F, Yang W, Wang H, et al. Community-based lung cancer screening of high-risk population with low-dose computed tomography in China. Ann Oncol 2017; 28:v502-6.
Kang HR, Cho JY, Lee SH, et al. Role of low-dose computerized tomography in lung cancer screening among never smokers. J Thorac Oncol. 2019; 14: 436-444.
Wang CL, Hsu KH, Chang YH, et al. Low-Dose Computed Tomography Screening in Relatives With a Family History of Lung Cancer. J Thorac Oncol 2023; 18:1492-1503.
Brodersen J, Voss T, Martiny F, et al. Overdiagnosis of lung cancer with low-dose computed tomography screening: meta-analysis of the randomised clinical trials. Breathe 2020; 16:200013.
Callister MEJ, Sasieni P, Robbins HA. Overdiagnosis in lung cancer screening. Lancet Respir Med 2021; 9:7-9.
Rendle KA, Saia CA, Vachani A, et al. Rates of Downstream Procedures and Complications Associated With Lung Cancer Screening in Routine Clinical Practice : A Retrospective Cohort Study. Ann Intern Med 2024; 177:18-28.
Clay R, Rajagopalan S, Karwoski R, et al. Computer Aided Nodule Analysis and Risk Yield (CANARY) characterization of adenocarcinoma: radiologic biopsy, risk stratification and future directions. Transl Lung Cancer Res 2018; 7:313-326.
Tammemagi M, Ritchie AJ, Atkar-Khattra S, et al. Predicting Malignancy Risk of Screen-Detected Lung Nodules-Mean Diameter or Volume. J Thorac Oncol 2019; 14:203-211.
hu W, Love K, Gray SW, Raz DJ. Liquid Biopsy Screening for Early Detection of Lung Cancer: Current State and Future Directions. Clin Lung Cancer 2023; 24:209-217.
Yang CJ, Wang H, Kumar A, et al. Impact of Timing of Lobectomy on Survival for Clinical Stage IA Lung Squamous Cell Carcinoma. Chest 2017; 152:1239-1250.
Ponholzer F, Kroepfl V, Ng C, et al. Delay to surgical treatment in lung cancer patients and its impact on survival in a video-assisted thoracoscopic lobectomy cohort. Sci Rep 2021; 11: 4914.